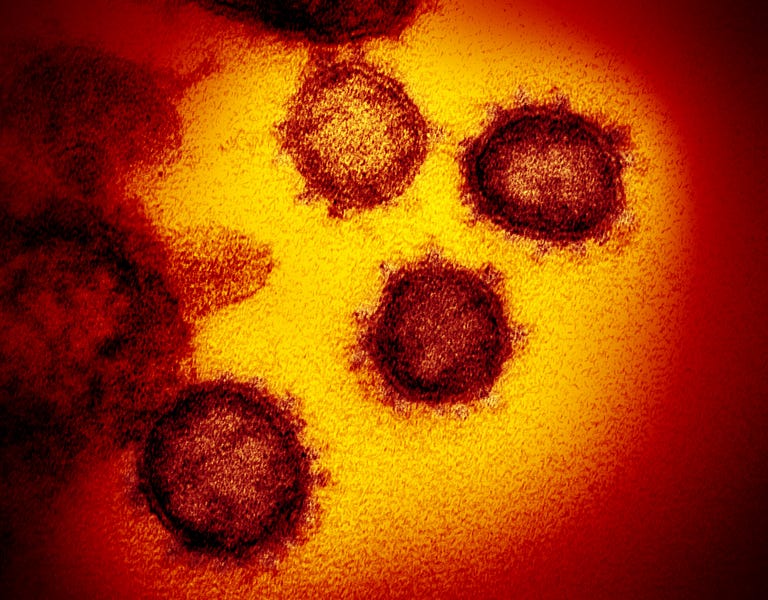
For months now, virologists and epidemiologists have been debating a simple question about COVID-19 transmission: How small does a particle exhaled by an infected person have to be before it’s too small to spread the virus? We know that ballistic droplets, the comparatively large globules expelled when breathing, speaking or singing that fall to the ground quickly, generally don’t travel farther than six feet, and are the basis of virus-fighting guidelines like social distancing and masking. But some scientists have argued for months that there’s evidence to suggest the virus that causes COVID can also hitch a ride on droplets small and light enough to hang in the air for hours, and that these “aerosols,” as they are called, might be a substantial contributor to the spread of the pandemic.
Back in July, the World Health Organization acknowledged that aerosols might play a role in spreading COVID: “We have to be open to this evidence and understand its implications regarding the modes of transmission.” Then, this past weekend, the CDC went even further. In a change to their online primer for how the coronavirus spreads, they described COVID-19 as an “airborne disease”—in other words, a disease transmitted primarily through aerosols.
“There is growing evidence that droplets and airborne particles can remain suspended in the air and be breathed in by others, and travel distances beyond 6 feet (for example, during choir practice, in restaurants, or in fitness classes),” the updated language read. “In general, indoor environments without good ventilation increase this risk.”
Soon after the change was released, however, the CDC abruptly changed tack, claiming the update had been posted in error. “Unfortunately an early draft of a revision went up without any technical review,” Jay Butler, the CDC’s deputy director for infectious disease, told reporters Monday.
What gives here? Simply saying ‘the CDC accidentally goofed and shared inaccurate information’ doesn’t do the story justice. Set aside the question of what breakdown in CDC processes led to it being posted prematurely online—someone at the CDC had to write that guidance. If it was wrong, why write it? If it was right, why back away from it?
Unpacking this requires us to take a step back. The first question isn’t “How did the CDC get itself in this messaging mess?” Rather, it’s “why hasn’t the CDC had anything to say about aerosol transmission before?” The central thesis of the now-retracted change in guidance, that “growing evidence” supports an aerosol transmission pathway for COVID-19, has been known for months. It’s the preeminent explanatory model for well-documented, otherwise inexplicable phenomena like COVID superspreader events and the virus being far more contagious indoors than out.
What’s particularly interesting is that the CDC and other federal public health authorities have previously acknowledged this likelihood of aerosol transmission of COVID—just not in such explicit terms. CDC guidance for minimizing the threat of COVID transmission at reopening businesses includes instructions to “consider taking steps to improve ventilation in the building” and to “improve central air filtration”—precautions that do absolutely nothing to inhibit ballistic spread, but are best practices for combatting aerosol transmission. Similarly, EPA guidelines on indoor air and coronavirus state that “when used along with other best practices … increasing ventilation can be part of a plan to protect yourself and your family.”
How, then, to explain the CDC’s reluctance to come right out and acknowledge that we appear to be dealing with aerosol/airborne transmission of the coronavirus?
One clue might be found in the EPA guidance mentioned above. Three separate EPA fact sheets mention air filtration and ventilation as tools to help inhibit the spread of COVID-19, and all three contain a version of the same caveat: “By itself, increasing ventilation is not enough to protect people from exposure to the virus that causes COVID-19.” Anti-aerosol measures, the government maintains, should only be taken in addition to the ordinary steps (masking, distancing, and the like) that are otherwise recommended to stop the spread of the coronavirus.
This framing highlights one of the biggest difficulties remaining in our understanding of COVID transmission: While it looks increasingly clear that both ballistic and aerosol transmission is taking place, we don’t know what proportion of cases are attributable to each. And what helps protect against the one isn’t the same as what protects against the other.
“There are implications—pretty significant ones—related to mask-wearing, for instance,” Dr. Jeff Niederdeppe, a Cornell professor of communication who teaches strategic health messaging, told The Dispatch. “What has kind of been the message that this is the best we can do, is wear masks—well, if aerosol transmission is responsible for a huge proportion of the cases, that directly undermines that kind of guidance.”
You can easily imagine a scenario, then, where the CDC is loath to explicitly describe COVID-19 as an “airborne disease” on the grounds that such language—even if true—might mislead people into thinking the anti-virus precautions to which we’ve become accustomed aren’t any use after all.
Of course, there’s also always the specter of outside interference to consider. The Trump administration has not exactly covered itself in glory when it comes to managing public health narratives during the pandemic, and in recent weeks has on several occasions been caught pressuring its public health experts to change health guidance to better fit their political aims.
Photograph by Image Point FR-LPN/BSIP/Universal Images Group/Getty Images.


Please note that we at The Dispatch hold ourselves, our work, and our commenters to a higher standard than other places on the internet. We welcome comments that foster genuine debate or discussion—including comments critical of us or our work—but responses that include ad hominem attacks on fellow Dispatch members or are intended to stoke fear and anger may be moderated.
With your membership, you only have the ability to comment on The Morning Dispatch articles. Consider upgrading to join the conversation everywhere.