Recently, the Dispatch Fact Check looked at a claim by Hillary Clinton that Donald Trump had cut CDC funding. While this was not true overall — despite the president’s proposed budgets containing cuts for the CDC, the bills that actually passed Congress included funding increases — Clinton had also claimed that Trump “cut back on this program of overseas vigilance” and we described that phrase as a truthful claim.
Since then, several outlets have published fact checks claiming that the CDC had not cut funding to overseas efforts to ward off pandemics. FactCheck.org ran a piece calling claims similar to Clinton’s “false” based on interviews with the CDC—though the claims they investigated were a bit more specific, as some public figures, including Senate Minority Leader Chuck Schumer, had stated that the CDC cut its work in foreign countries from 49 to 10 nations.
We decided that the confusion warranted further reporting.
In February 2014, 10 countries led by the United States and the CDC launched a five-year initiative called the Global Health Security Agenda. The world had experienced a number of epidemics in the preceding 15 years, from SARS in 2002 to Ebola in 2014, and, realizing that epidemic control needed to be a global effort, the countries came together to ensure that the world would be better prepared for future infectious diseases. The United States provided funding and non-monetary support from the start. The funding was made possible through a five-year emergency package given to the CDC and the United States Agency for International Development during the Ebola epidemic that ran out in September 2019.
Through the GHSA, the CDC supported 17 Phase I countries and 28 Phase II countries—14 individual countries, plus CARICOM, an organization of Caribbean countries. One CARICOM country, Haiti, received individual support from the CDC as a Phase II country, while the rest were treated as a region rather than separate countries for GHSA purposes. The phase distinctions were made based on identified shortfalls in countries’ health security capacities—Phase I countries being those in more need of assistance.
Both Phase I and II countries received technical assistance from the CDC, while Phase I countries also received direct financial support. Collectively, these 45 countries, with four additional countries that house CDC-sponsored Global Disease Detection Centers, comprised what was termed “global health security priority countries” in an academic paper put out by the CDC. It appears it was activities in these 49 countries that news outlets like the New York Times, the Wall Street Journal, and the Washington Post were referring to when they wrote in early 2018 that the CDC would be cutting back on epidemic preparedness activities in 39 out of the 49 countries where it had a presence.
At the end of 2017, shortly before the impending cuts were announced, the CDC had helped fund national lab systems in nine of the Phase I countries, expanded disease surveillance and reporting systems in 10, and had trained field-based epidemiologists in all 17 Phase I countries.
While Phase II countries were not directly given money, the CDC still supported such nations by providing “country capacity assessments, five-year roadmaps, and annual GHSA implementation plan development” and other technical assistance.
In light of the coronavirus, much attention has been paid to the U.S. government’s response and the aforementioned reporting that the CDC was scaling back epidemic activities overseas. The 2018 reporting was cited in recent articles by the New York Times, Business Insider, and even here at The Dispatch, among other outlets. The FactCheck.org piece on the subject included a statement from CDC associate director for Global Health Security Maureen Bartee, disputed that the CDC had actually “cut back its work from 49 to 10 countries.” Here’s Bartee’s full statement:
In fiscal year 2020, the U.S. government, including CDC, is working with 19 priority partner countries to build preparedness and capacity to prevent, detect, and respond to infectious disease threats at their source. These countries are Bangladesh, Burkina Faso, Cameroon, Cote D’Ivoire, Democratic Republic of the Congo (DRC), Ethiopia, Guinea, India, Indonesia, Kenya, Liberia, Mali, Nigeria, Pakistan, Senegal, Sierra Leone, Tanzania, Uganda, and Vietnam. In addition to these 19, CDC is supporting global disease detection, emergency and humanitarian response, and other global health protection activities in Cambodia, China, Egypt, Georgia, Ghana, Guatemala, Kazakhstan, Kyrgyzstan, Mexico, Niger, Panama, South Africa, South Korea, Thailand, Ukraine and Uzbekistan.
Also, CDC is establishing platforms with regional offices to advance global health security and maintain a sustainable global presence. With this regional approach, CDC intends to implement a sustainable, long-term overseas operational structure, expand the reach of its technical assistance and programs, and strengthen disease outbreak response. CDC is currently establishing regional platforms in South America (Brazil), Eastern Europe/Central Asia (Georgia), Middle East/North Africa (Oman), and Southeast Asia (Vietnam).
Beyond those countries listed here, CDC, along with other U.S. government agencies, continues to support a broad range of global health programs (e.g., HIV/AIDS, malaria, tuberculosis, global immunization) that address global infectious diseases threats, as well as response to major outbreaks that require international assistance. All told, CDC is currently working in more than 60 countries.
FactCheck.org concluded: “With its current funding, Bartee said, the CDC is actually working in ‘more than 60 countries’—not 10—to address the threat of global infectious diseases and outbreaks.” However, Bartee uses very general language in her statement, and reaches the ultimate “60 countries” figure by lumping together all CDC work in foreign countries instead of focusing on the Global Health Security Agenda’s epidemic preparedness activities.
FactCheck.org states, as further proof that the cuts did not end up happening, that “CDC operating budget plans show that its funding for global public health protection—which includes global disease detection and emergency response and global public health capacity—increased from $58 million in fiscal year 2017 to around $108 million in fiscal years 2018 and 2019. (And that does not include any remaining supplemental funds available for use.)”
The increase, however, was known at the time the cuts were announced, and was specifically mentioned in a New York Times article about the CDC cutting back overseas. The issue, as stated in the Times article, was that the increase was not enough to maintain programs in foreign countries at the levels they had been.
The Global Health Technologies Coalition, a global health advocacy group, published an article in late March 2018, after fiscal year 2018’s budget was passed and echoed the Times article: The budget included “a substantial increase of $50 million for global health security programming, which supports implementation of the Global Health Security Agenda (GHSA),” but “more funding is still needed to sustain these programs.”
When announcing the launch of the GHSA, the United States committed “to invest more than $1 billion in resources to expand the Global Health Security Agenda.” The bulk of that funding came from $909 million allocated to the CDC and the United States Agency for International Development as a part of the five-year emergency Ebola package. (The agencies received more in funds as a part of the package, but the rest of the money was earmarked for other purposes.) Together, the CDC and USAID’s global health security budget in 2015, the year the GHSA was launched, totaled $1.0366 billion.
(These statistics are pulled from a table compiled by the Kaiser Family Foundation, a health care policy nonprofit. The table includes the Department of Defense’s budgets for its Biological Threat Reduction Program and Global Emerging Infections Surveillance and Response System. The DoD programs’ funding have been ignored for the purposes of this article.)
In 2016, USAID received an additional one-time grant of $145.5 million for global health security as a part of an emergency package to combat the Zika virus. Since the packages were allotted only once, their impact on the global health security budget is not reflected in following years; so though the 2017 global health security budget appears lower than the past two years at $130.7 million, it doesn’t take into account funds still being spent from the Ebola and Zika packages. In 2018 and 2019, an additional $100 million and $38 million, respectively, were allotted to global health security through USAID from leftover Ebola funds initially planned for other expenses. In addition to the one-time grants, USAID provides tens of millions of dollars annually to global health programs annually.
Taking all sources of funding into account, the CDC’s global health security budget averaged out to $393.5 million annually from 2015-2019. The Ebola and Zika packages increased the budget for global health security an average of $238.5 million a year, meaning without them the annual global health security budgets would average $155 million, of which the CDC contributed an average of $76.98 million with the rest coming from USAID. So while the CDC’s budget increases from $58.2 million to $108.2 million in 2018 and from $108.2 million to $183 million in fiscal year 2020 seem like a big deal, the increases still aren’t enough to make up for the loss of $238.5 million in additional funding that the emergency packages provided from 2015-2019, even including the $100 million in funds USAID budgeted for global health security in 2020.
In a 2017 report titled “Healthier World, Safer America,” PATH, a global health nonprofit, suggested that even with Ebola package funds base appropriation levels for the CDC and USAID needed to increase in order to sustain their global health security work over the next three years. PATH estimated the CDC would have to increase its global health security budget to $208.2 million annually and USAID would need to up its contributions to $172.5 million. Since the CDC’s budget request and USAID’s budget request include $175 million and $115 million respectively for global health security in fiscal year 2021, the shortfall is unlikely to be addressed in the near future.
Health and Human Services Deputy Secretary Eric Hargan did announce at the end of 2018 that the United States would commit $150 million to the GHSA to support the organization’s 2024 target, but the extra $150 million over spread over the course of several years puts the total budget still well below Ebola-package levels.
It is true that the CDC did not “cut back its work from 49 to 10 countries” as Bartee says, but given the decrease in available funds the United States is not capable of operating at the same level it once did in global health security priority countries. The CDC does not share many details about where the money in their budget ends up going, so it’s hard to quantify decreases in countries where the CDC is still active. However, a CDC representative provided materials to The Dispatch showing where the CDC is active globally in 2020: a map of countries that received programmatic assistance from the CDC and a more general list of countries that includes those that receive even just minimal assistance.
The list of countries that receive global health protection support from the CDC consists of 74 countries in total, but a CDC representative cautioned that “support could be as minimal as a visit from CDC to conduct training, to having CDC staff in-country on a daily basis to assist the country’s ministry of health in addressing its public health priorities.”
The lack of differentiation based on levels of support makes it impossible to determine which countries receive regular support from the CDC. The list is further problematic because it refers to “global health protection,” a category which encompasses more than the Global Health Security Agenda programs in question. Given the list’s lack of details, it is an imperfect resource for determining which GHSA global health security priority countries the CDC still supports in epidemic prevention efforts. Nevertheless, 12 of the 49 global health security priority countries don’t appear on it at all, meaning they no longer receive even occasional, minimal support from the CDC. Based on other available resources, it seems likely that the CDC has ended regular support for even more countries.
The map the CDC provided, titled “2020 CDC Global Presence & Programmatic Activities,” also uses broad categorization, referring to “global health protection.” The map also includes some countries that Bartee did not list, while leaving out some that she did. After inquiries from the Dispatch Fact Check about discrepancies between the map and what Bartee told FactCheck.org, a CDC representative responded, “The map has some errors and we are working to get it updated.” The updated map is not expected to be ready for six weeks, leaving Bartee’s list in the FactCheck.org interview the only CDC-approved resource for determining which GHSA countries the CDC still supports more than minimally.
Bartee listed 19 “priority partner” countries that she specifically mentions the CDC assists in epidemic activities, along with a second, more general grouping of 16 countries the CDC supports in “global disease detection, emergency and humanitarian response, and other global health protection activities.” As with the list and map, it’s not possible to tell which countries the CDC provides with epidemic support.
“The U.S. Centers for Disease Control and Prevention (CDC) does not maintain a list that distinguishes countries receiving epidemic support from those receiving emergency and humanitarian support,” Bartee said in an email to The Dispatch.
While at least 12 global health security priority countries, and likely more, no longer receive assistance from the CDC, it is not apparent that remaining countries are supported at the same level they were before the five-year emergency package funds ran out in 2019. Reuters, for example, reported recently a CDC-employed epidemiologist left her job in China last July after learning her position would be cut in September—the same month that the five-year emergency package ended. She was responsible for training field epidemiologists, health officials responsible for detecting diseases and tracking them to their source of origin to contain them in order to prevent pandemics.
It isn’t possible to confirm exact numbers, but with everything considered, it seems our earlier fact check—and reporting from 2018—is likely correct: The CDC did indeed “end epidemic prevention activities” in GHSA-supported countries, curtailing them in some while ceasing them completely in others.
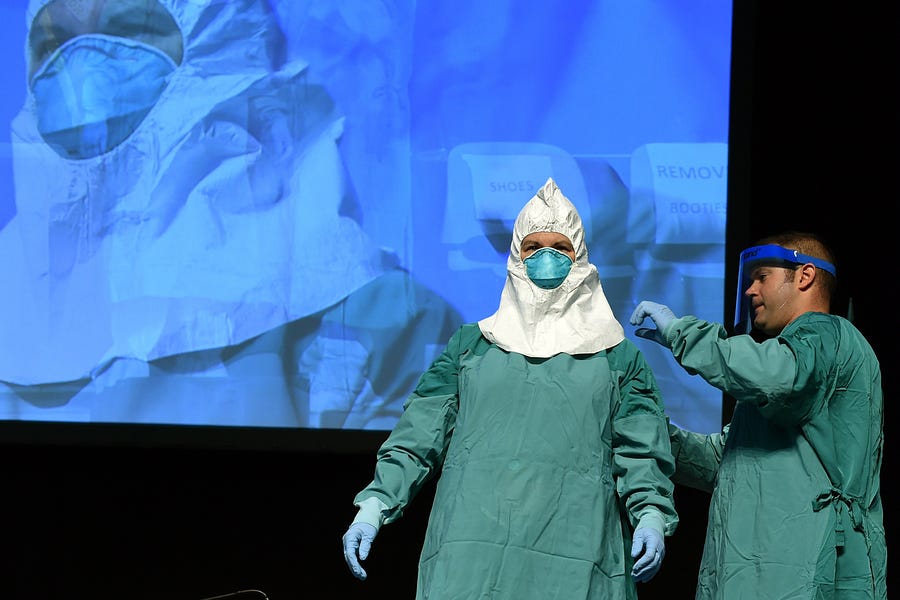
Photograph of a CDC-led training session for health care workers on Ebola virus preparations in October 2014 by Timothy A. Clary/AFP/Getty Images.
If you have a claim you would like to see us fact check, please send us an email at factcheck@thedispatch.com. If you would like to suggest a correction to this piece or any other Dispatch article, please email corrections@thedispatch.com





Please note that we at The Dispatch hold ourselves, our work, and our commenters to a higher standard than other places on the internet. We welcome comments that foster genuine debate or discussion—including comments critical of us or our work—but responses that include ad hominem attacks on fellow Dispatch members or are intended to stoke fear and anger may be moderated.
With your membership, you only have the ability to comment on The Morning Dispatch articles. Consider upgrading to join the conversation everywhere.