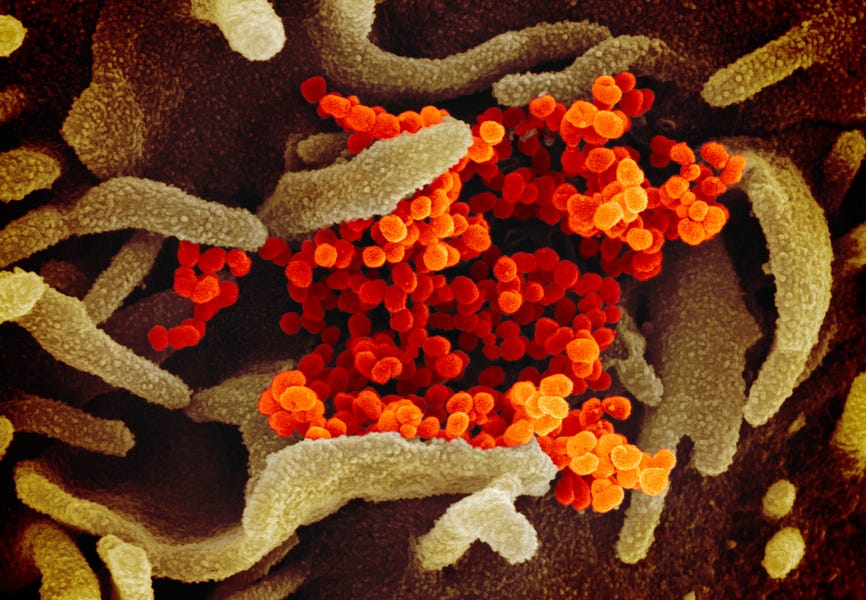
A retweet by President Trump last weekend set off a storm of misinformation about coronavirus deaths and takes advantage of confusion about the concept of “comorbidity” and how death certificates are filled out.
Trump retweeted a post from a QAnon supporter that claimed, “This week the CDC quietly updated the Covid number to admit that only 6% of all the 153, 504 deaths actually died from Covid, that’s 9210 deaths. The other 94% had 2-3 other serious illnesses and the overwhelming majority were of very advanced age.”
Twitter eventually deleted the Tweet for violating its rules. But the message had already gone viral. Trump and his campaign legal adviser, Jenna Ellis, both retweeted a Gateway Pundit article on the same claim, and Grace Community Church pastor John McArthur declared, “There is no pandemic.”
So, what’s actually going on? First, the CDC’s website, as updated on August 26, does indeed say “For 6% of the deaths, COVID-19 was the only cause mentioned.” The text is an introduction to a table on comormidities, and explains that for the other deaths, there was an average of “2.6 additional conditions or causes per death.”
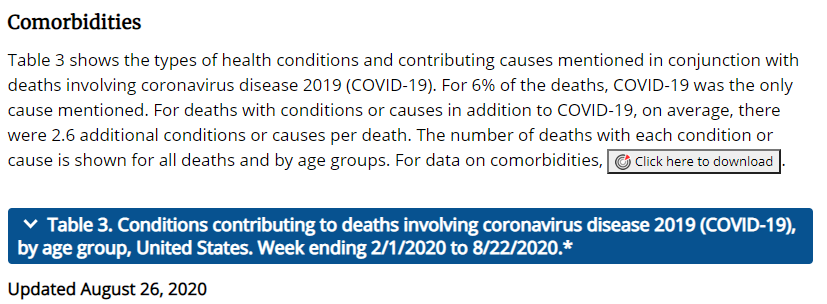
Before going any further let’s quickly dispense with one bit of disinformation, the claim that the website was “quietly updated.” Prior versions of the page also contain a “comorbidities” section, and the Washington Post linked to the May version of the chart. So, this is not actually sudden breaking news.
The CDC page also mentions that the death counts are based on death certificate data, and understanding how death certificates are filled out, and the differences between terms like “immediate cause” and “underlying cause” helps paint a much clearer picture. It’s also important to note that the conditions that contribute to patient deaths and appear on the death certificate are not always the preexisting conditions that make some Americans more vulnerable to COVID.
Here’s a hypothetical scenario that is based on a few COVID-19 cases I have seen myself as a physician:
A 75-year-old male, who is known to have coronary artery disease (CAD) and chronic obstructive pulmonary disease (COPD), is brought to the emergency room with a fever, and trouble breathing. His COVID-19 PCR test is positive, and his chest X-ray is consistent with viral pneumonia. He is admitted to the hospital, and he slowly improves over a week.
But just as doctors are discussing a possible discharge, he clutches his chest, and says “Doc, I can’t breathe.” As COVID-19 is known to cause blood clots, the doctors suspect a pulmonary embolism (blood clot in the lung), and rush to get a CT scan of his chest, which confirms a blood clot exists. Unfortunately, before they can start blood thinners, the patient stops breathing and loses his pulse (cardio-pulmonary arrest). Despite full resuscitation efforts, the patient cannot be revived and is pronounced dead.
And now his doctor has to fill out a death certificate. If that happened to be me, how would I do it?
So, here is a picture of the medical portion of a standard paper death certificate. (It should be noted that nowadays most are actually filled out online).
Per CDC guidance, I know that the “immediate cause of death, which is the disease or condition that directly precedes death and is not necessarily the underlying cause of death (UCOD),” should be reported on Line A. The conditions that led to the immediate cause of death should be reported in a logical sequence in terms of time and etiology below it.” (The underlying cause of death is listed last in the sequence, and is defined by the World Health Organization as the disease or injury that “initiated the train of events leading directly to death.”
While some of my colleagues would report “cardio-pulmonary arrest” as the “immediate cause”, the CDC death certificate instructions actually state “the terminal event (cardiac arrest or respiratory arrest) should NOT be used.” I’d therefore write “pulmonary embolism” on Line A. As blood clots in the lungs usually don’t initially form in the lungs but travel up from clots (thrombi) in the legs, I would write “presumed deep venous thrombosis of lower extremity” on Line B. As this likely would not have occurred if the patient wasn’t “hypercoagulable” (meaning he had a condition that made blood more likely to clot), I’d write “hypercoagulable state” on Line C. Finally, as the underlying cause of death, that which caused the hypercoagulable state, I’d write “COVID-19” on Line D.
But I’m not done yet. Remember, the patient in the scenario also had a history of CAD and COPD, and it’s very likely both contributed to the death. If the patient hadn’t had heart disease, maybe his heart wouldn’t have stopped, even with a pulmonary embolism. If the patient hadn’t had COPD, the damage to his lungs from the virus may not have been as bad, and the patient might have kept breathing despite the clot. Also, the CDC actually instructs me that:
In some cases, survival from COVID-19 can be complicated by pre-existing chronic conditions, especially those that result in diminished lung capacity, such as chronic obstructive pulmonary disease (COPD) or asthma. These medical conditions do not cause COVID-19, but can increase the risk of contracting a respiratory infection and death, so these conditions should be reported in Part II.
So, I’d add that below:
Now, here’s an example of a death certificate from the CDC itself:
In this case, a 77-year-old male with hypertension and COPD presented with fever, cough, shortness of breath, and wheezing. He had a positive COVID-19 test, and had severe respiratory acidosis; a condition in which the patient is unable to exhale carbon dioxide well, and the carbon dioxide builds up in the blood to the point it becomes acidotic, and this eventually kills him. The certificate therefore lists the respiratory acidosis as the immediate cause of death, “due to” COVID-19.
But, COPD can also cause respiratory acidosis, an hence is mentioned under “significant conditions contributing to death.” However, COPD cannot directly cause COVID-19, although it can “increase susceptibility to or exacerbate an infection”, and this is why COVID-19, not COPD, is the “underlying cause of death.”
Even in the case of a patient who had no chronic medical conditions, it would be rare to list only COVID-19 as a cause of death. Here’s another scenario:
In this case, a previously healthy 34-year-old female is diagnosed with COVID-19 via PCR. A CT scan reveals viral pneumonia; she eventually develops acute respiratory distress syndrome and dies.
So, the only type of patient where COVID-19 would be the ONLY cause of death mentioned on a death certificate, would be a previously perfectly healthy one with no medical conditions whatsoever, who had a positive COVID-19 test, but suddenly died before any other tests could be performed to diagnose other conditions.
President Trump has a well-documented history of trying to downplay the severity of the pandemic, so it is perhaps unsurprising that he and his supporters would try to seize on a statistic that shows there have been only about 9,000 COVID deaths. But that misinformation obscures a much more revealing statistic.
The CDC reports that “when COVID-19 appears on a death certificate, it’s the underlying cause for more than 95 percent of those deaths.” And as for those claims that people who die “with COVID” are listed as dying “from COVID”? The CDC acknowledges that “in some cases, COVID-19 may have contributed to the death, but the underlying cause was another, such as terminal cancer”; that is, the patient died with COVID, but from the cancer. The percentage of cases is less than 5 percent.
Photograph by Image Point/BSIP/Universal Images Group via Getty Images.




Please note that we at The Dispatch hold ourselves, our work, and our commenters to a higher standard than other places on the internet. We welcome comments that foster genuine debate or discussion—including comments critical of us or our work—but responses that include ad hominem attacks on fellow Dispatch members or are intended to stoke fear and anger may be moderated.
You are currently using a limited time guest pass and do not have access to commenting. Consider subscribing to join the conversation.
With your membership, you only have the ability to comment on The Morning Dispatch articles. Consider upgrading to join the conversation everywhere.